







Ordre des Médecins du Hainaut
Docteur Jacques Bruart
Président
Rue des Archers 6B
7000 Mons
Bruxelles, le 06/06/2023
Chers confrère,
Vous trouverez ci-joint un article co-écrit en 2021 concernant l’augmentation potentielle de l’efficacité du « vaccin » Covid par l’apport de certains aliments, apports micro nutritionnels (vit D, Zinc, etc.), activité physique, non tabagisme, etc.
A l’époque, SOUS RESERVE DE TESTS CLINIQUES AVEC UNE REELLE PHASE 2 SUIVIE D’UNE VRAIE PHASE 3 sur quelques milliers de volontaires rémunérés pour le risque encouru (et non pas en prenant des milliards de rats de laboratoires à leur insu par ruse), nous étions complètement favorables à cette option. Cette phase test est non réalisable en 8 mois (il faut une dizaine d’années)(*), et aucune thérapie par ARN messager n’avait abouti après 25 ans de recherche…
Nous savions déjà par exemple de très longue date que l’efficacité du vaccin grippe (et les anticorps générés) baissait avec l’âge : ceci étant expliqué par la chute des taux de Zinc (malabsorption intestinale), des taux de vit D (moindre exposition soleil), chute de synthèse de la DHEA (il existe encore actuellement en 2023 des médecins ne s’inquiètent pas de cette DHEA !)
Vous constaterez donc que je suis absolument PRO VAX ….. jusqu’à ce que les faits et les chiffres nous démontrent que ce « vaccin » n’a aucune caractéristique d’un vaccin, et de plus dans la plupart des catégories d’âge : le bénéfice risque est complètement inversé , surtout dès la 2 et 3-ème injection : réaction facilitante ADE. Une scientifique de renom, spécialiste du RNA avait prédit avant la sortie de ce « vaccin » la problématique.
La seule catégorie d’âge encore douteuse actuellement est celle des plus de 65 ans avec comorbidités : le risque des mourir des effets secondaires du vaccin pourrait être inférieur au bénéfice apporté par celui-ci .
Oserais-je rappeler que officiellement (et l’ordre des médecin n’a émis aucune objection), sans qu’il y ait la moindre étude, on encourage la vaccination des enfants, des femmes enceintes. Pfizer lui-même déconseille cette vaccination aux femmes enceintes !
Confraternellement
Dr Résimont
(*) et aucune urgence de trouver une thérapie nouvelle puisque déjà en Avril 2020, des molécules connues pouvaient être utilisées (mais pas de brevet, donc pas de possibilité de plantureux bénéfices et pots de vin pour sponsoriser les politiques, leurs conseillers dits « experts » et les revues scientifiques inféodées à l’industrie).
Increasing Efficacy of Covid-19 Vaccines by Lifestyle Interventions
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with, the contents by NLM or the National Institutes of Health.
2022 Oct; 77(5): 1527–1538.
Abstract
COVID-19 caused a serious threat to the world population as it spread worldwide rapidly. Existing medicines and vaccines could not cure and control this deadly disease. In this regard, several vaccines have been proposed and designed to control this infection’s spread effectively. Along with these vaccines, the general population should adopt specific lifestyle interventions to strengthen their immune system and combat deadly viruses. We used Google Scholar and PubMed databases to find the related information using key terms such as ‘COVID-19’, ‘COVID-19 AND Vaccine efficacy’, ‘Lifestyle intervention AND COVID-19’, and « Lifestyle intervention AND Vaccines, » etc. Only articles that discussed the interactions between lifestyle intervention and the efficacy of COVID-19 vaccines were selected for this study. Several previous clinical trials and scientific observations with influenza, polio, and other viral vaccines have demonstrated that vaccine response varies across individuals for antibody titer, independent of vaccine antigenicity. This different vaccine response observed among individuals is attributed to several factors such as dietary and nutritional habits, physical activity, stress and sleep deprivation, deficiency of micronutrients (minerals, vitamins), gut microbiota composition, immunosenescence, smoking, and drinking habits. Although there is not much information about COVID-19 vaccine efficacy and lifestyle interventions, experience with other vaccines can undoubtedly be used to suggest lifestyle interventions to improve COVID-19 vaccine efficacy.
These lifestyle interventions may boost antibody responses against COVID-19 vaccines, leading to higher protection from the disease, especially among elderly and immunocompromised people. In conclusion, the present review attempts to understand the role of various nutritional and psychological factors that lead to poor vaccine response and suggests specific nutritional and psychological interventions that can enhance vaccine efficacy and improve immune response against COVID-19 vaccines.
Keywords: Vaccine Efficacy, COVID-19, SARS-CoV-2, Lifestyle interventions, Micronutrients, Sleep Deprivation, Stress
1. Context
Humans have greatly benefited from developing safe and efficacious vaccines against several diseases. The widespread use of vaccines in various public health programs has significantly reduced the mortality and morbidity associated with various diseases and has saved 6 million people annually ( 1 , 2 ). In the past few decades, scientists have successfully developed and introduced vaccines for diseases like diphtheria, hepatitis, influenza, measles, pneumococcal disease, poliomyelitis, and rabies. Vaccines for other diseases are also « in the pipeline » ( 1 ). Coronavirus disease 2019 (COVID-19), a global pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus has taken thousands of human lives globally with 241,411,380 confirmed cases and 4,912,112 confirmed deaths due to SARS-CoV-2 having been reported as of September 2021 ( 3 ). COVID-19 has created an alarming health situation, and a successful fight against this global pandemic requires urgent steps toward finding efficacious treatment options and developing protective and preventive strategies ( 3 ). Due to their proven track record against viral diseases, vaccines are an obvious preventive and protective strategy against COVID-19. SARS-CoV-2 is a positive-strand RNA coronavirus of the Coronaviridae family and shares close genetic similarities with other members of the Coronaviridae family, namely, severe acute respiratory syndrome (SARS) and the Middle East respiratory syndrome (MERS). Some of the most suggested antigenic molecules encoded by the genome of these viruses are structural proteins such as spike (S) protein, envelope (E) protein, membrane (M) protein, and nucleocapsid (N) proteins that can target the development of vaccines against the virus. However, most vaccines have been targeted against the S-protein, preventing virus entry into the host cell and viral infection ( 4 ). As per the WHO (World Health Organization) report, 79 COVID-19 vaccine candidates were under clinical trial as of March 5, 2021, with 12 vaccine candidates having already entered phase III clinical trial and four more in phase IV clinical trial. In addition, around 182 vaccine candidates were under preclinical development.
Interestingly, more than 90% of the most promising candidates have been designed for intramuscular delivery ( 5 ). An ideal COVID-19 vaccine candidate must protect the vaccinated, including immunocompromised individuals, from infection and disease, should be able to offer long-term memory immune response, and must be reproduced in billions of numbers. These characteristics urge the need for immediate and large-scale production of vaccines against COVID-19 ( 6 ). Significantly, vaccine efficacy depends not only on the vaccine but also on factors specific to the vaccinated individual. Several scientific studies have demonstrated that robust vaccine response depends on psychological factors. Individuals suffering from poor psychological health due to depression, stress, and loneliness show impaired immune functions, leading to reduced vaccine efficacy, with the elderly being the most vulnerable group ( 7 – 9 ).
The association between vaccine efficacy and other nutritional and psychological factors is crucial in the COVID-19 vaccines. Therefore, the present review explores the available scientific evidence demonstrating an association between lifestyle factors and vaccine efficacy. Since scientific studies relating to COVID-19 and lifestyle factors/interventions are very limited, we have used the available scientific literature for other vaccine candidates to put forward the point that vaccine efficacy can be increased by incorporating particular lifestyle and nutritional interventions into our daily lives.
2. Evidence Acquisition
We used Google Scholar and PubMed databases to find the related information using key terms such as « COVID-19 », « COVID-19 AND Vaccine efficacy », « Lifestyle intervention AND COVID-19′, and « Lifestyle intervention AND Vaccines, » etc. This study only included articles that discussed the interactions of lifestyle interventions with the efficacy of COVID-19 vaccines.
3. Results
3.1. Nutritional Habits
Nutritional habits play a crucial role in maintaining a healthy immune system, and adequate nutrition is essential to reduce the risk of various infections caused by viruses, bacteria, and parasites. For example, vitamins (C, D), zinc, selenium, and proteins play a crucial role in normal immune system functioning and boosting immunity against infectious diseases ( 10 ). Given the crucial role of nutritional habits in shaping the immune response, adequate nutritional interventions that show beneficial effects on the immune system are essential to combat the COVID-19 pandemic ( 11 ). At the same time, carefully chosen nutritional interventions may be used to enhance vaccine efficacy against COVID-19 without causing any significant change in lifestyle and diet. For instance, Low, Rutherfurd ( 12 ) reported increased humoral response in BALB/c mice fed with whey protein concentrate (WPC) against influenza and poliomyelitis vaccines, diphtheria, and tetanus toxoids, and ovalbumin and cholera toxin subunits. The WPC-fed mice displayed a higher intestinal tract, and serum antibody response within 2 weeks of immunization for all antigens than the control group fed a standard chow diet. Although the WPC-fed group showed a higher primary and secondary intestinal-tract antibody response, the only secondary serum antibody response was higher in the WPC-fed group. The study demonstrated that WPC could be used as a nutritional intervention to improve vaccine efficacy for various antigenic molecules ( 12 ).
A controlled, randomized, double-blind pilot study conducted on 21 healthy elderly (>60 years of age) individuals showed that dairy protein treated with ultraviolet-C (UV-C) light was more effective in enhancing vaccine response against DTaP vaccine than dairy protein subjected to pasteurization process ( 13 ). The antibody response of unheated dairy protein was also higher than the control soy protein after 8 weeks. The results of this study suggest that incorporating UV-C treated dairy protein (unheated protein) may help individuals overcome immunosenescence ( 13 ). There are comprehensive scientific studies to show that nutritional habits such as increased intake of the western diet (a diet characterized by higher omega-6 and lower omega-3 and increased use of salt and refined sugar) caused chronic-low grade inflammation by promoting the secretion of several inflammatory cytokines such as TNF (tumor necrosis factor)-alpha, IL (interleukin)-17, CRP (C reactive proteins) and adversely impact immunity, liver, kidneys, and heart ( 14 ).
Since systemic inflammation has been linked to a reduced immune response against vaccines, maintaining a healthy diet may aid vaccine efficacy ( 15 ). Obesity, a direct consequence of overnutrition and poor dietary habits, has been shown to reduce vaccine response. This observation is critical given that globally, 36.9% of men and 38.0% of women are obese, thus putting around 1/3rd of the global population at risk for poorvaccine response against COVID-19 vaccines ( 16 ). Mainly, obese individuals show higher morbidity and mortality from COVID-19 compared to normal subjects, and lower vaccine efficacy among obese subjects is a significant cause for concern ( 17 ).
3.2. Micronutrient’s Supplementation
The role of micronutrients in improving vaccine efficacy has been well reported in several clinical trials ( 18 , 19 ). Although clinical data that shows a strong association between COVID-19 vaccines and micronutrients are minimal, studies with other vaccines have shown that lifestyle interventions in the form of improved nutrition can significantly increase the overall antibody response against a vaccine. For instance, 83 healthy subjects of the 65–85-year age group in the Ageing and Dietary Intervention Trial either took low fruit and vegetables (≤2 FV portions/day) or higher (≥5 FV portions/day) for 16 weeks ( 20 ). In the 12thweek, all participants received intramuscular tetanus toxoid (0.5 mL) and Pneumovax II vaccine (0.5 mL). At the 16th week, a specific antibody response against tetanus (total IgG) and Pneumovax II (total IgG and IgG2) was measured. It was observed that participants taking higher FV intake (≥5 FV portions/day) had higher levels of antibodies binding the pneumococcal capsular polysaccharide (IgG) than participants with lower FV intake (≤2 FV portions/day). However, no significant difference in antibody response was observed against the tetanus toxoid. This study concludes that increased FV intake can improve vaccine efficacy against the Pneumovax II vaccine in older people and may be used as a dietary intervention to augment the immune response to vaccines ( 20 ).
Vitamin D is considered a vital immunomodulator, and its deficiency is associated with immune dysregulation and heightened inflammation. Notably, the presence of vitamin-D receptors on immune cells (B & T cells, monocytes, dendritic cells) and the ability of the immune cells to locally convert inactive vitamin D to active vitamin D clearly shows that vitamin D plays an instrumental role in maintaining the healthy immune system ( 21 ). Interestingly, higher serum levels of vitamin D (>30 ng/mL) were associated with reduced COVID-19 PCR positivity, lower CRP and D-dime levels, and reduced lung damage, indicating lower COVID-19 severity in individuals with higher vitaminD status ( 22 ). In a recent study, Chiu, Tsai ( 23 ) advocated using vitaminD to improve the COVID-19 vaccine efficacy. Clinical trials to understand the impact of vitamin D on the COVID-19 vaccine are underway (24). COVID-19 vaccine response includes neutralizing antibodies and specific CD4+ and CD8+ T-cell responses against the SARS-CoV-2 ( 24 ). In another important clinical observation, vitamin D deficient COVID-19 subjects showed reduced CD8+ T-cells and CD4/CD8 ratio ( 25 ). Therefore, studying the association between vitamin D and COVID-19 vaccine efficacy is undoubtedly beneficial in improving vaccine efficacy, especially in immunocompromised and immunosuppressed patients. Contrary to the above findings, a systematic review considering nine studies and a combined 2367 patients found no significant association between immune response against influenza vaccine and vitamin D levels, except a higher seroprotection observed against H3N2 and B strains in subjects with normal vitamin D levels than a subject with vitamin D deficiency ( 26 ). In another clinical observation, elderly subjects were given a complete liquid nutrition diet containing energy, minerals, vitamins, and antioxidants for 7 months and vaccinated against various influenza strains such as A/Sydney/5/97 (SY), A/Beijing/262/95 (BE), and B/Yamanashi/166/98 (YA). In this study, the strain-specific antibody response was observed, and using a liquid nutritional diet might have improved protection against the influenza vaccine by generating an increased antibody response ( 27 ).
Like vitamins, the role of minerals is also crucial in maintaining a healthy immune response in the body, and immune system enhancing roles of zinc ( 28 ) and calcium ( 29 ) are well reported. A randomized, double-blind, placebo-controlled study involving 53 subjects (aged ≥65 year) found zinc deficiency (<70 μg/dL) in 58% (n=31) of participants ( 30 ). The zinc-deficient subjects were either given lower zinc supplements (n=15; 5 mg Zn/day) or higher zinc (n=16; 30 mg Zn/day). As expected, the zinc supplementation for 3 months improved zinc levels by 16% more than the placebo group. Interestingly, zinc supplementation significantly increased T-cells proliferation stimulated by anti-CD3/CD28 and phytohemagglutinin, and a higher number of peripheral T-cellswere reported in such subjects. Higher T-cell functions observed upon zinc supplementation were mainly attributed to increased T-cells ( 30 ).
Similarly, calcium has been shown to improve immunity against viral infections by increasing glucose utilization in T-cells and consequently increasing T-cell multiplication ( 31 ). All-trans-retinoic acid (ATRA) protects against viruses entering the mucosal routes. At the molecular level, ATRA administration in mice increased the intestinal mucosal immunity against the lymphocytic choriomeningitis virus glycoprotein (LCMVgp) (Ad5gp) by increasing the number of both effector and memory T-cells, suggesting that ATRA may act as an adjuvant to improve memory T-cell response against viral pathogens (HIV) entering via mucosal membranes, and may aid in increasing vaccine efficacy ( 32 ). Glutathione (GSH) is another micronutrient proposed to benefit COVID-19 patients due to its antiviral properties and inhibitory effect on IL-6 in patients suffering from HIV and TB ( 33 ). Figure 1 summarizes how micronutrients maintain a healthy immune system and increase vaccine efficacy.
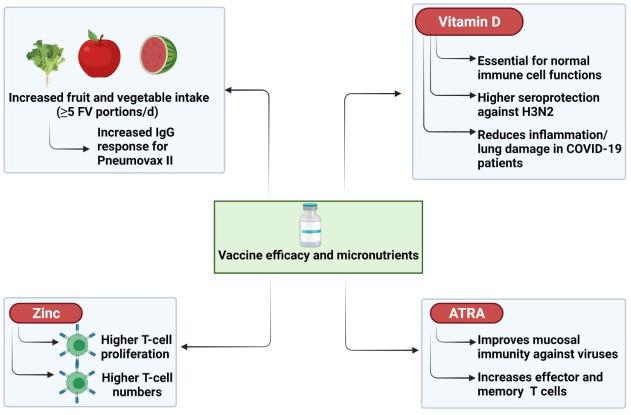
The impact of micronutrients on maintaining the normal immune response
Essential micronutrients such as minerals and vitamins are essential for normal immune cell function and, therefore, help in normal vaccine response. For instance, fruits and vegetables increased antibody response against the Pneumovax II vaccine. Vitamin D is a known immunomodulator and has been shown to protect lung damage in COVID-19 patients, and increase seroprotection for H3N2 vaccines. All-trans retinoic acid (ATRA) improved mucosal immunity and increases the number of effector and memory T-cells. Finally, minerals such as zinc help in maintaining the normal functions of T-cells. The use of micronutrients as a dietary intervention may help increase vaccine efficacy, including COVID-19, especially in immunocompromised individuals.
3.3. Physical Activity
Exercise exerts a direct and beneficial effect on the immune system. Immunosenescence is a significant decline in the overall functioning of the immune system cells and a shift in the leukocyte subpopulations. Factors such as aging, lower physical activity, reduced muscle mass, and malnutrition contributes to immunosenescence, leading to increased infection risk, lower vaccine efficacy, and higher risk for autoimmune disorders and cancer ( 34 ). Regular physical activity delays immunosenescence as it improves T-cell proliferation and functions, reduces the number of senescent T-cells, lowers the levels of inflammatory mediators, enhances NK (nature killer)-cell activity, and positively affects the vaccine response ( 35 ), as shown in figure 2. Although data regarding COVID-19 vaccine efficacy and exercise has not yet surfaced, studies with influenza vaccine have shown that regular exercise improves vaccine efficacy by eliciting increased antibody response against the vaccine. Notably, a poor immune response against the vaccine is a « hallmark of immunosenescence, » Therefore, increased physical activity can be used as an essential lifestyle intervention to enhance vaccine efficacy.
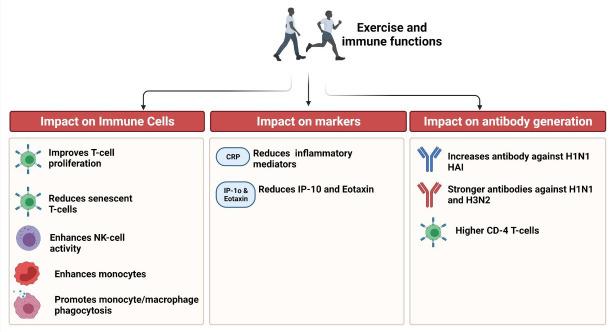
Association between physical activity and immune response
Physical activity directly affects immune cell activity, antibody generation, and inflammation. It improves immune cell functions by increasing proliferation, cytotoxic activity, and phagocytosis. Physical activity also reduced inflammation by reducing C-reactive protein levels and also reduces IP-10 and eotaxin levels. In certain studies, physical activity has been positively associated with increased antibody generation against viral vaccines.
A study in the Singaporean Chinese cohort (n=56) showed that participants who walked more displayed a higher number of monocytes and plasmablasts, increased expression of genes involved in monocyte/macrophage phagocytosis, and reduced levels of IP-10 and Eotaxin. Notably, a positive correlation between monocyte response and antibody response against H1N1 HAI was observed. In addition, the physically active women showed higher antibody response during the second follow-up conducted after 18 months, suggesting a positive correlation between physical activity and vaccine response ( 36 ). In a similar observation, elite athletes given influenza vaccine displayed increased CD4+ T-cell levels than the control group. In the elite athlete group, CD4+ T-cell levels increased 4.1-fold, while the control group showed a 2.3-fold rise in the CD4+T-cells post-vaccination.Post-vaccination, the T-cells were more restricted in their cytokine profile and showed a significantly higher expression of CTLA-4; again, the effects were more in the athlete group. Further, athletes showed more robust antibodies against H1N1 (swine flu) and H3N2, indicating that physical training led to a higher vaccine response in the athlete group than in the control group ( 37 ).
In contrast, a study conducted on Sixty-seven volunteers aged between 18-30 years did not find a significant association between antibody response against H1 (A/Texas/36/91) and H3 (A/Johannesburg/33/94) and physical activity or physical fitness ( 38 ). Valenzuela, Simpson ( 39 ) have also summarized the benefits of physical exercise on vaccine response citing several prior peer-reviews studies. They have opined that physical exercise may be a « coadjuvant treatment » for COVID-19. However, the strategies used to deliver COVID-19 vaccines differ from the influenza vaccines, making it difficult to generalize the benefits of physical exercise on COVID-19 vaccine efficacy ( 39 ). It is pertinent to mention that the Singapore government does not recommend strenuous physical activity post-vaccination for oneweek post-vaccination due to increased risk for heart problems, especially among people aged <30 years. There are reports that COVID-19 vaccines may increase the risk for myocarditis and pericarditis, leading to heart attacks in individuals involved in strenuous physical activity ( 40 ).
3.4. Stress and Sleep Interventions
Sleep and circadian rhythm have a strong influence on normal immune system functioning. While the levels of naive T-cells and production of pro-inflammatory cytokines peak during the early nocturnal sleep, the levels of NK cells and anti-inflammatory cytokines peak during daytime wakefulness ( 40 ). The number of nTreg (Natural T regulatory) fluctuates with the circadian rhythm and shows the highest number (mean 95 nTreg/µl) at night time and the lowest number (mean 55 nTreg/µl) during the daytime. In addition, the highest suppressive activity of nTreg was observed at 02.00 h, a lower activity at 15.00 h, and no activity at 07.00 h. Sleep deprivation significantly reduced CD4+CD25– T cell proliferation, disturbing the functional rhythm of CD4+CD25– T cells ( 41 ). Sleep deprivation also reduces the ability of T-cells to attach to virus-infected cells, a process mediated by T-cell receptor (TCR) induced activation of β2-integrins.
In contrast, normal sleep upregulated antiviral functions of T-cells by upregulating integrin activation compared to nocturnal wakefulness ( 42 ). Research studies correlating COVID-19 vaccine efficacy and sleep deprivation have not yet emerged, but existing studies with other vaccines have shown that sleep deprivation lowers vaccine efficacy. A study on 11 male and 13 female subjects who received the H1N1 vaccine showed that sleep-deprived males developed lower antibodies against the H1N1 vaccine, with no effect observed in females. Interestingly, the impact of sleep deprivation on antibody generation was not different at later time points. This important observation suggests that adequate sleep is essential for a normal antibody response against the vaccine (influenza) during the early stage of the adaptive immune response. Sleep deprivation may not have a lasting impact on antibody titer against the influenza vaccine ( 43 ).
Like sleep, stress is also a significant psychological factor in mounting immune response against a vaccine (Figure 3). Several scientific studies have established that psychological stress adversely affects normal immune cell functions and vaccine response ( 44 ). Interestingly, short-term stress (minutes to hours) enhances innate immunity by increasing the immune cell activity, maturation, and function and changing the secretion of cytokines. However, long-term stress leads to immune dysregulation by adversely affecting the number and maturation of immune cells and causing a disruption in Type 1-Type 2 cytokine balance ( 45 ). In a cohort of 83 healthy young adults, the antibody response was measured at baseline, 1-month, and 4-month and correlated with salivary cortisol levels.
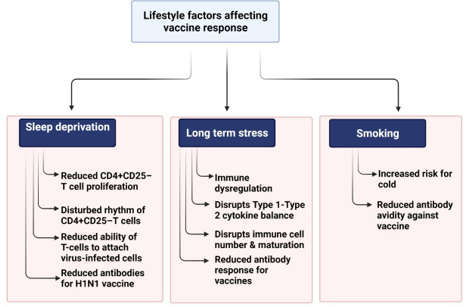
Lifestyle factors such as sleep deprivation, stress, and smoking habits adversely impact immune cell functions and hence may lead to poor vaccine response
Sleep deprivation has been shown to disrupt normal circadian rhythm. It also reduces CD4+CD25– T cell proliferation lowers the ability of T-cells to attach with the virus-infected cells, and reduces antibody response for the H1N1 vaccine. Stress is known to disrupt immune cell proliferation, immune cell numbers, immune cell maturation, cause Type 1-Type 2 cytokine imbalance, and lower the vaccine response. Smoking is known to increase cold risk and reduce the avidity of antibodies.
Interestingly, increased stress lowered the humoral immune response against the New Caledonia strain vaccine, as reflected by reduced antibody titer ( 46 ). Sleep increases growth hormone and prolactin levels at the hormonal level and reduces cortisol levels. This hormonal modulation improves the crosstalk between antigen-presenting cells and (Ag)-specific T helper (Th) cells, leading to higher adaptive immune response and antibody titer against the antigen ( 47 ). While the association between sleep and vaccine efficacy may not cause much difference for most healthy people, advising adequate/extended sleep may be helpful in immunocompromised people in improving vaccine response for COVID-19 vaccines ( 48 ).
3.5. Microbiota Interventions
Vaccine immunogenicity is highly variable among individuals and different populations. In addition, suboptimal vaccine efficacy has been observed among vulnerable populations such as infants, the elderly, and individuals living in lower-and-middle income countries. Recent scientific evidence from several human and animal models have demonstrated a direct association between human microbiota composition and antibody response against vaccine ( 49 ). Recently revised estimates suggest that the number of human microbiotas is the same as the total human cells. In a “reference man” of 7 kg, the total mass of microbial cells is around 0.2 kg ( 50 ). Healthy microbiota is essential for normal immune cell functioning because germ-free mice have shown a reduced number of plasma and T-cells and underdeveloped Peyer’s patches ( 51 ). A study in the mice model has demonstrated that well-developed gut microbiota is essential for eliciting normal antibody response against the trivalent inactivated influenza (TIV) vaccine. TIV vaccination to mice deficient in toll-like receptors (Trl5−/− mice) resulted in fewer plasma cells and reduced antibody titers. However, the antibody response was restored when flagellated Escherichia coli, but not flagellated, was given to animals. The improved antibody response is mainly attributed to TLR5-mediated sensing of flagellin, which leads to the differentiation of plasma cells and releases the plasma cell growth factors from lymph node macrophages. However, the impact of microbiota on antibody response was not the same for other vaccines. For instance, microbiota impacted antibody response against inactivated polio vaccine, but no impact was observed against adjuvant vaccines or the live-attenuated yellow fever vaccine ( 52 ).
Another study in the mice model showed that antibiotic-driven intestinal dysbiosis during early life impaired normal antibody response against five vaccines: Bexsero, NeisVac-C, Prevenar, INFANRIX Hexa, and the BCG. However, the impaired antibody response was rescued when the commensal gut microbiota was restored. Interestingly, the impaired antibody response against vaccines was not observed in antibiotic-treated adult mice, suggesting that gut dysbiosis induced by antibiotics in the early-life can potentially modulate vaccine efficacy against some of the most commonly used vaccines in infants worldwide ( 53 ).
Given the crucial role of gut microbes in eliciting normal humoral responses against vaccines, probiotics have gained attention to improve vaccine efficacy. A systematic review found the beneficial effect of probiotics on vaccine response against oral vaccinations and for parenteral influenza vaccination, indicating that probiotics may be used as a low-cost intervention to enhance vaccine response. However, the study variable factors, such as probiotic strain, dosing, duration, and timing of administration, must be considered before reaching any definitive conclusion ( 54 ). Another systematic review involving 20 RCTs comprising 1979 adults observed that probiotics or prebiotics significantly improved the seroprotection rate for H1N1 and H3N2 strains, while a higher seroconversion rate was reported for the B strain. The study observes that probiotics and prebiotics improve influenza vaccine efficacy by directly impacting seroprotection and seroconversion ( 55 ).
3.6. Other Lifestyle Habits
Besides nutritional and psychological factors, lifestyle habits such as smoking and alcohol consumption also affect immunity and vaccine response (Figure 3). For instance, Cohen, Tyrrell ( 56 ) reported a higher risk for common cold among smokers than non-smokers, and smokers are more vulnerable to infection and subsequent illness after infection. However, the study reported a reduced risk for cold among moderate alcohol drinkers (3-4 drinks/day), with no impact on clinical illness observed among smokers. In a pilot study to evaluate the impact of smoking on vaccine antibody response, 104 non-smoking and 112 smoking female participants were vaccinated at 0, 1, and 6 months using Cervarix™ and HAVRIX™ vaccines. It was observed that both non-smokers and smokers had comparable levels of HPV16/18 antibodies response against vaccines at 7 months. However, smokers (cotinine level > 20 ng/ml) showed a 3-times higher risk for developing lower avidity HPV16/18 IgG antibodies, suggesting that smoking may not impact the number of antibodies elicited by vaccines. However, its adversary impacts the avidity of IgG generated in response to HPV16/18 vaccination ( 57 ). Another important lifestyle factor that affects vaccine response is alcohol consumption. Interestingly, the impact of alcohol consumption on immunity is driven mainly by the quantity of alcohol consumed. It has been observed that higher alcohol consumption reduces the immune response and raises the risk for infectious diseases. In contrast, moderate consumption of polyphenol-rich alcohol benefits the immune system. However, the findings cannot be generalized, and factors such as alcohol quantity, gender, and the pattern of alcohol consumption may also be considered to determine the impact of alcohol consumption on the immune system ( 58 ).
A study in rhesus macaques investigated the impact of ethanol consumption on antibody response against the Modified Vaccinia Ankara (MVA) vaccine and observed that animals with blood ethanol concentration (BEC) greater than 80 mg/dl showed reduced vaccine response as reflected by lower levels of IgG and reduced CD4+ and CD8+ T cell proliferation than control animal. However, moderate drinkers whose BEC remained below 80 mg/dl showed a solid CD8+ T cell response and produced more robust MVA-specific antibodies than the control group. Cytokine profiling showed higher levels of antiviral cytokines and elevated expressions of microRNAs involved in CD8+ T cell differentiation in the moderate group ( 59 ). It is important to mention that although some scientific data support that moderate alcohol consumption is beneficial for immunity and may increase the immune response against vaccines, the number of such studies is still a handful. Notably, alcohol consumption cannot be recommended to boost the immune response against COVID-19 because this could be harmful to the most vulnerable groups such as infants, the elderly, immunocompromised people, and individuals already suffering from alcohol use disorders.
4. Conclusion
The development of vaccines against COVID-19 in such a short time frame is a remarkable scientific achievement and made possible by intense efforts of the scientific community, aided by freely available scientific literature, and massive funding from private consortia and governments. However, the availability and distribution of the COVID-19 vaccine to the global population remain challenging. Notably, the vaccine response in vaccinated individuals does not remain the same due to certain individual-specific psychological, nutritional, and lifestyle habits. The present review summarizes some scientific studies that associate lifestyle habits with vaccine efficacy. Clinical studies have established that vaccine antibody response can be augmented by reducing stress, sleeping for adequate periods, incorporating sufficient micronutrients (vitamins and minerals) in the diet, lowering alcohol consumption, and avoiding cigarette smoking. Based on available studies with other vaccines and considering the imminent need to tackle the COVID-19 pandemic, it is prudent to learn from past scientific studies and propose specific nutritional and lifestyle interventions to boost the immune response against COVID-19 vaccines. However, the lack of scientific trials that associate lifestyle, nutrition, and psychological behavior with COVID-19 vaccine efficacy present an opportunity for the scientific community to explore this area because the outcomes will significantly impact the formulation of better vaccination policies against COVID-19.
Authors’ Contribution
Study concept and design: A. G.
Acquisition of data: P. K. M.
Analysis and interpretation of data: S. N.
Drafting of the manuscript: S. P.
Critical revision of the manuscript for important intellectual content: A. G. and S. R.
Administrative, technical, and material support: A. G. and A. M.
Articles from Archives of Razi Institute are provided here courtesy of Razi Vaccine and Serum Research Institute
References
3. Khan S, Siddique R, Bai Q, Liu Y, Xue M, Nabi G, et al. Coronaviruses disease 2019 (COVID-19): causative agent, mental health concerns, and potential management options. J Infect Public Health. 2020 [PMC free article] [PubMed] [Google Scholar]
4. WHO. COVID-19 weekly epidemiological update, edition 58, 21 September 2021. 2021 [Google Scholar]
5. Calina D, Docea AO, Petrakis D, Egorov AM, Ishmukhametov AA, Gabibov AG, et al. Towards effective COVID-19 vaccines: Updates, perspectives and challenges. Int J Mol Med. 2020;46(1):3–16. [PMC free article] [PubMed] [Google Scholar]
6. Kyriakidis NC, López-Cortés A, González EV, Grimaldos AB, Prado EO. SARS-CoV-2 vaccines strategies: a comprehensive review of phase 3 candidates. NPJ Vaccines. 2021;6(1):1–17. [PMC free article] [PubMed] [Google Scholar]
7. Madison AA, Shrout MR, Renna ME, Kiecolt-Glaser JK. Psychological and behavioral predictors of vaccine efficacy: Considerations for COVID-19. Perspect Psychol Sci. 2021;16(2):191–203. [PMC free article] [PubMed] [Google Scholar]
8. Jabaaij L, Grosheide P, Heijtink R, Duivenvoorden H, Ballieux R, Vingerhoets A. Influence of perceived psychological stress and distress on antibody response to low dose rDNA hepatitis B vaccine. J Psychosom Res. 1993;37(4):361–9. [PubMed] [Google Scholar]
9. Pandey K, Thurman M, Johnson SD, Acharya A, Johnston M, Klug EA, et al. Mental Health Issues During and After COVID-19 Vaccine Era. Brain Res Bull. 2021;176:161–73. [PMC free article] [PubMed] [Google Scholar]
10. Trichet VV. Nutrition and immunity: an update. Aquac Res. 2010;41(3):356–72. [Google Scholar]
12. Low P, Rutherfurd K, Gill H, Cross M. Effect of dietary whey protein concentrate on primary and secondary antibody responses in immunized BALB/c mice. Int Immunopharmacol. 2003;3(3):393–401. [PubMed] [Google Scholar]
13. Schaefer S, Hettinga KA, Cullor J, German JB, Henrick BM. Use of UV treated milk powder to increase vaccine efficacy in the elderly. Front Immunol. 2018;9:2254. [PMC free article] [PubMed] [Google Scholar]
15. Pereira B, Xu X-N, Akbar AN. Targeting inflammation and immunosenescence to improve vaccine responses in the elderly. Front Immunol. 2020;11:2670. [PMC free article] [PubMed] [Google Scholar]
17. Popkin BM, Du S, Green WD, Beck MA, Algaith T, Herbst CH, et al. Individuals with obesity and COVID‐19: A global perspective on the epidemiology and biological relationships. Obes Rev. 2020;21(11):e13128. [PMC free article] [PubMed] [Google Scholar]
18. Isanaka S, Garba S, Plikaytis B, Malone McNeal M, Guindo O, Langendorf C, et al. Immunogenicity of an oral rotavirus vaccine administered with prenatal nutritional support in Niger: a cluster randomized clinical trial. PLoS Med. 2021;18(8):e1003720. [PMC free article] [PubMed] [Google Scholar]
19. Drakesmith H, Pasricha S-R, Cabantchik I, Hershko C, Weiss G, Girelli D, et al. Vaccine efficacy and iron deficiency: an intertwined pair? . Lancet Haematol. 2021;8(9):e666–e9. [PMC free article] [PubMed] [Google Scholar]
20. Gibson A, Edgar JD, Neville CE, Gilchrist SE, McKinley MC, Patterson CC, et al. Effect of fruit and vegetable consumption on immune function in older people: a randomized controlled trial. Am J Clin Nutr. 2012;96(6):1429–36. [PubMed] [Google Scholar]
22. Demir M, Demir F, Aygun H. Vitamin D deficiency is associated with COVID‐19 positivity and severity of the disease. J Med Virol. 2021;93(5):2992–9. [PMC free article] [PubMed] [Google Scholar]
23. Chiu S-K, Tsai K-W, Wu C-C, Zheng C-M, Yang C-H, Hu W-C, et al. Putative Role of Vitamin D for COVID-19 Vaccination. Int J Mol Sci. 2021;22(16):8988. [PMC free article] [PubMed] [Google Scholar]
24. Inserra F, Tajer C, Antonietti L, Mariani J, Ferder L, Manucha W. Vitamin D supplementation: An alternative to enhance the effectiveness of vaccines against SARS-CoV-2? . Vaccine. 2021;39(35):4930. [PMC free article] [PubMed] [Google Scholar]
25. Ricci A, Pagliuca A, D’Ascanio M, Innammorato M, De Vitis C, Mancini R, et al. Circulating Vitamin D levels status and clinical prognostic indices in COVID-19 patients. Respir Res. 2021;22(1):1–8. [PMC free article] [PubMed] [Google Scholar]
26. Lee M-D, Lin C-H, Lei W-T, Chang H-Y, Lee H-C, Yeung C-Y, et al. Does vitamin D deficiency affect the immunogenic responses to influenza vaccination? A systematic review and meta-analysis. Nutrients. 2018;10(4):409. [PMC free article] [PubMed] [Google Scholar]
27. Wouters-Wesseling W, Rozendaal M, Snijder M, Graus Y, Rimmelzwaan G, De Groot L, et al. Effect of a complete nutritional supplement on antibody response to influenza vaccine in elderly people. J Gerontol A Biol Sci Med Sci. 2002;57(9):M563–M6. [PubMed] [Google Scholar]
28. Shankar AH, Prasad AS. Zinc and immune function: the biological basis of altered resistance to infection. Am J Clin Nutr. 1998;68(2):447S–63S. [PubMed] [Google Scholar]
29. Vaeth M, Eckstein M, Shaw PJ, Kozhaya L, Yang J, Berberich-Siebelt F, et al. Store-operated Ca2+ entry in follicular T cells controls humoral immune responses and autoimmunity. Immunity. 2016;44(6):1350–64. [PMC free article] [PubMed] [Google Scholar]
30. Barnett JB, Dao MC, Hamer DH, Kandel R, Brandeis G, Wu D, et al. Effect of zinc supplementation on serum zinc concentration and T cell proliferation in nursing home elderly: a randomized, double-blind, placebo-controlled trial. Am J Clin Nutr. 2016;103(3):942–51. [PubMed] [Google Scholar]
31. Vaeth M, Maus M, Klein-Hessling S, Freinkman E, Yang J, Eckstein M, et al. Store-operated Ca2+ entry controls clonal expansion of T cells through metabolic reprogramming. Immunity. 2017;47(4):664–79. [PMC free article] [PubMed] [Google Scholar]
32. Tan X, Sande JL, Pufnock JS, Blattman JN, Greenberg PD. Retinoic acid as a vaccine adjuvant enhances CD8+ T cell response and mucosal protection from viral challenge. J Virol. 2011;85(16):8316–27. [PMC free article] [PubMed] [Google Scholar]
33. Guloyan V, Oganesian B, Baghdasaryan N, Yeh C, Singh M, Guilford F, et al. Glutathione supplementation as an adjunctive therapy in COVID-19. Antioxidants. 2020;9(10):914. [PMC free article] [PubMed] [Google Scholar]
35. Simpson RJ, Lowder TW, Spielmann G, Bigley AB, LaVoy EC, Kunz H. Exercise and the aging immune system. Ageing Res Rev. 2012;11(3):404–20. [PubMed] [Google Scholar]
36. Choon Lim Wong G, Narang V, Lu Y, Camous X, Nyunt MSZ, Carre C, et al. Hallmarks of improved immunological responses in the vaccination of more physically active elderly females. Exerc Immunol Rev. 2019;25 [PubMed] [Google Scholar]
37. Ledo A, Schub D, Ziller C, Enders M, Stenger T, Gärtner BC, et al. Elite athletes on regular training show more pronounced induction of vaccine-specific T-cells and antibodies after tetravalent influenza vaccination than controls. Brain Behav Immun. 2020;83:135–45. [PubMed] [Google Scholar]
38. Schuler P, Lloyd L, Leblanc P, Clapp T. The effect of physical activity and fitness on specific antibody production in college students. J Sports Med Phys Fitness. 1999;39(3):233. [PubMed] [Google Scholar]
39. Valenzuela PL, Simpson RJ, Castillo-García A, Lucia A. Physical activity: A coadjuvant treatment to COVID-19 vaccination? Brain Behav Immun. 2021 [PMC free article] [PubMed] [Google Scholar]
41. Bollinger T, Bollinger A, Skrum L, Dimitrov S, Lange T, Solbach W. Sleep‐dependent activity of T cells and regulatory T cells. Clin Exp Immunol. 2009;155(2):231–8. [PMC free article] [PubMed] [Google Scholar]
42. Dimitrov S, Lange T, Gouttefangeas C, Jensen AT, Szczepanski M, Lehnnolz J, et al. Gαs-coupled receptor signaling and sleep regulate integrin activation of human antigen-specific T cells. J Exp Med. 2019;216(3):517–26. [PMC free article] [PubMed] [Google Scholar]
43. Benedict C, Brytting M, Markström A, Broman J-E, Schiöth HB. Acute sleep deprivation has no lasting effects on the human antibody titer response following a novel influenza A H1N1 virus vaccination. BMC Immunol. 2012;13(1):1–5. [PMC free article] [PubMed] [Google Scholar]
44. Seiler A, Fagundes CP, Christian LM. The impact of everyday stressors on the immune system and health. Stress Challenges and Immunity in Space : Springer; 2020. [Google Scholar]
45. Dhabhar FS. Effects of stress on immune function: the good, the bad, and the beautiful. Immunol Res. 2014;58(2):193–210. [PubMed] [Google Scholar]
46. Miller GE, Cohen S, Pressman S, Barkin A, Rabin BS, Treanor JJ. Psychological stress and antibody response to influenza vaccination: when is the critical period for stress, and how does it get inside the body? . Psychosom Med. 2004;66(2):215–23. [PubMed] [Google Scholar]
49. Lynn DJ, Benson SC, Lynn MA, Pulendran B. Modulation of immune responses to vaccination by the microbiota: implications and potential mechanisms. Nat Rev Immunol. 2021:1–14. [PMC free article] [PubMed] [Google Scholar]
51. Pabst O, Hornef M. Gut microbiota: a natural adjuvant for vaccination. Immunity. 2014;41(3):349–51. [PubMed] [Google Scholar]
52. Oh JZ, Ravindran R, Chassaing B, Carvalho FA, Maddur MS, Bower M, et al. TLR5-mediated sensing of gut microbiota is necessary for antibody responses to seasonal influenza vaccination. Immunity. 2014;41(3):478–92. [PMC free article] [PubMed] [Google Scholar]
53. Lynn MA, Tumes DJ, Choo JM, Sribnaia A, Blake SJ, Leong LEX, et al. Early-life antibiotic-driven dysbiosis leads to dysregulated vaccine immune responses in mice. Cell Host Microbe. 2018;23(5):653–60. [PubMed] [Google Scholar]
54. Zimmermann P, Curtis N. The influence of probiotics on vaccine responses–A systematic review. Vaccine. 2018;36(2):207–13. [PubMed] [Google Scholar]
55. Lei W-T, Shih P-C, Liu S-J, Lin C-Y, Yeh T-L. Effect of probiotics and prebiotics on immune response to influenza vaccination in adults: a systematic review and meta-analysis of randomized controlled trials. Nutrients. 2017;9(11):1175. [PMC free article] [PubMed] [Google Scholar]
56. Cohen S, Tyrrell D, Russell MA, Jarvis MJ, Smith AP. Smoking, alcohol consumption, and susceptibility to the common cold. Am J Public Health. 1993;83(9):1277–83. [PMC free article] [PubMed] [Google Scholar]
57. Namujju PB, Pajunen E, Simen-Kapeu A, Hedman L, Merikukka M, Surcel H-M, et al. Impact of smoking on the quantity and quality of antibodies induced by human papillomavirus type 16 and 18 AS04-adjuvanted virus-like-particle vaccine–a pilot study. BMC Res Notes. 2014;7(1):1–6. [PMC free article] [PubMed] [Google Scholar]
58. Romeo J, Wärnberg J, Nova E, Díaz LE, Gómez-Martinez S, Marcos A. Moderate alcohol consumption and the immune system: a review. Br J Nutr. 2007;98(S1):S111–S5. [PubMed] [Google Scholar]
59. Messaoudi I, Asquith M, Engelmann F, Park B, Brown M, Rau A, et al. Moderate alcohol consumption enhances vaccine-induced responses in rhesus macaques. Vaccine. 2013;32(1):54–61. [PMC free article] [PubMed] [Google Scholar]